Homework 4: Risk
Homework objectives
Use these problems to practice Risk analysis, including, where appropriate, ARR, RRR, Odds, and NNT (or NNH)
Homework 4 expectations
BI-311 students: For homework reports, report only your answers for the even numbered questions. Read through the entire homework before starting to answer a question — all questions are intended to help you achieve the learning outcomes for the chapter. You are expected to have read the chapter and to have completed preceding homework. Answers are provided to numbered odd problems — turn in your work for even numbered problems.
How to work this homework
You may work together, but each of your must turn in your own report. Don’t “plagiarize” from each other. Do include in your report who you worked with.
What to turn in: A pdf file containing your answers to the even-numbered questions and relevant R code; by relevant we mean include your code, not copies of code provided to you. For statistical results, report appropriate significant figures. Use of RMarkdown recommended — because it is a simple way to include graphs generated; however copy/paste into a word document, then converted to pdf, is also acceptable.
Notes. By relevant we mean provide just the R code and results from R functions necessary to support your answers to the questions. For example, do not include
- the entire data set when head(dataset) will do
- screenshots of R output!! R output is text — copy/paste
- all statistical output from an R function.
See Part09: Making a report for an example homework file.
Submit your work to CANVAS. Obey proper file naming formats.
Resources for this homework
Mike’s Biostatistics Book: Chapter 7
Mike’s Workbook for Biostatistics: A quick look at R and R Commander, Part01 – Part10 and previous homework pages presented in this workbook.
RcmdrPlugin.EBM can help with some of the calculations. See Chapter 7.4 in Mike’s Biostatistics Book.
Additional R commands and or code provided below.
Questions
1. Sensitivity of a test is defined as
- False Positive Rate
- True Positive Rate
- False Negative Rate
- True Negative Rate
2. Specificity of a test is defined as
- False Positive Rate
- True Positive Rate
- False Negative Rate
- True Negative Rate
3. In thinking about the results of a test of a null hypothesis, Type I error rate is equivalent to
- False Positive Rate
- True Positive Rate
- False Negative Rate
- True Negative Rate
4. What is the primary outcome of screening (eg, mammogram for breast cancer, fecal immunochemical test for colorectal cancer), for evidence of cancer?
- Five-year survival rate after diagnosis
- Mortality rate after diagnosis
- Presence of cancer
- Positive or negative screening result
5. Both odds and relative risk are used to quantify association between an exposure and an outcome. The two are not identical, however. When the outcome is rare, odds and relative risk will yield similar conclusions. When outcome is common, results of odds and relative risk calculations may lead to drastically different conclusions. For each of the three designs listed below (A,B,C), identify whether odds, relative risk, or both can be used
- Case-control retrospective study
- Cohort prospective study
- Randomized control trial
Hint: Which type of study is the number of exposed subjects unknown?
6. Chromosome mutations are surprisingly frequent in human reproduction. The estimated distribution of chromosome mutations among all human conceptions that develop sufficiently to implant in the uterus is 8%. Among live births, 0.61% have chromosomal abnormalities. The most accurate test for chromosomal mutations requires amniocentesis. Amniocentesis carries a risk of miscarriage, about 1 in 200 (about 200K procedures annually, per Mayo Clinic; a recent systematic review places the risk at about 15 in 2000 procedures, per Akolekar et al 2015). What is the chance that a pregnancy that is miscarried due to amniocentesis actually has a chromosome abnormality?
7. Detection of Down syndrome requires acquisition of fetal cells, and the standard method is amniocentesis. Amniocentesis — like any invasive medical procedure — carries a risk of miscarriage. How risky? Difficult to know for any particular hospital or doctor, but the national rate is about 1 in 200 procedures (about 200K procedures annually, per Mayo Clinic; a recent systematic review places the risk at about 15 in 2000 procedures, per Akolekar et al 2015). Risk of chromosomal abnormalities increases with maternal age. Thus, decision to be tested must involve a weighing of risks: Risk of chromosomal abnormalities to the fetus and increasing maternal age vs. risk of amniocentesis and spontaneous miscarriage. A graph is shown below (Fig 1, data from CDC), which characterizes the risk to the fetus by maternal age and in the context of live births by maternal age category.
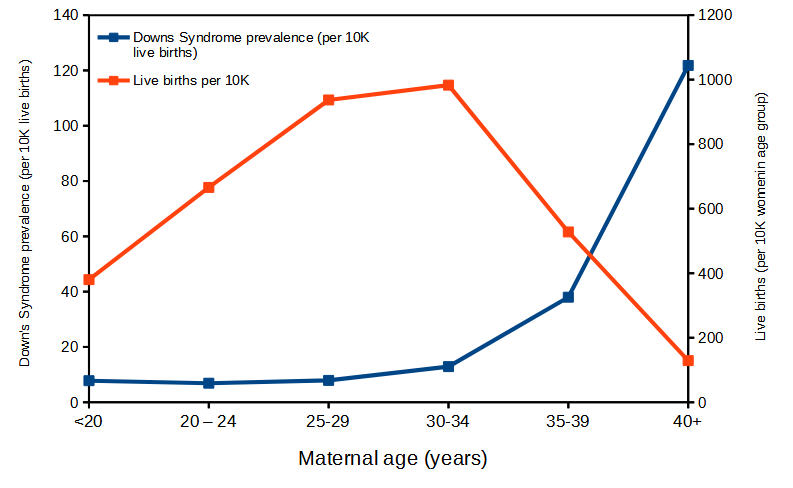
Figure 1. Live births (red) and Down’s Syndrome (blue) per 10,000 women by maternal age groups. In 2010, about 4 million live births of an estimated 6.2 million pregnancies. Non live births include 1.1 million induced abortions and 1.05 million fetal losses. Data from CDC
At what maternal age is the number needed to harm NNH approximately equal to 100? To 200? (NNH is the same concept as NNT, but instead of “treat” we write “harm” and infer risk of spontaneous miscarriage due to amniocentesis).
8. Women’s Health Initiative study investigated benefits and risks of replacement estrogen therapy in women (data derived from Figure 2, Manson et al 2013). The incidence of breast cancer in the treatment group (conjugated equine estrogens and medroxyprogesterone acetate) was 206 per 8506 women. The incidence in the placebo group was 155 per 8102 women. What was the Relative Risk Reduction, Absolute Risk Reduction, NNT, and Odds ratio?
9. Cases were men and women diagnosed with oral–oesophageal cancer in relation to coffee drinking habits. Data were from a cohort, prospective study of Norwegian men and women between age 40 – 45 followed for about a decade (data derived from Table 1 and Table 2, Tverdal et al 2011 – numbers reported in this table were not adjusted for possible confounding variables — see Tverdal et al for complete analysis).
|
|
Oral–oesophageal cancer | ||
|
Cups of coffee per day |
Cases | Noncases |
Total |
| < 1 cup | 35 | 41,419 |
41,454 |
|
1 or more cups |
415 |
347,755 |
348,170 |
| Total | 450 | 389,174 | 389,624 |
Does coffee drinking increase risk of oral cancer? Calculate the Relative Risk Reduction (and Odds ratio), Absolute Risk Reduction, and NNH.
10. The sensitivity of the fecal occult blood test (FOBT) is reported to be 0.68. What is the False Negative Rate?
11. The specificity of the fecal occult blood test (FOBT) is reported to be 0.98. What is the False Positive Rate?
12. For men in the United States between 50 and 54 years of age, the rate of colon cancer is 61 per 100,000. If the false negative rate of the fecal occult blood test (FOBT) is 10%, how many persons who have colon cancer will test negative?
13. For men in the United States between 50 and 54 years of age, the rate of colon cancer is 61 per 100,000. If the false positive rate of the fecal occult blood test (FOBT) is 10%, how many persons who do not have colon cancer will test positive?
14. A study was conducted to see if mammograms reduced mortality
| Deaths/1000 women | |
| No mammogram | 4 |
| Mammogram | 3 |
What is the RRR?
15. A study was conducted to see if mammograms reduced mortality
| Deaths/1000 women | |
| No mammogram | 4 |
| Mammogram | 3 |
What was the NNT?
16. Does supplemental Vitamin C decrease risk of stroke in Type II diabetic women? A study conducted on 1,923 women, a total of 57 women had a stroke, 14 in the normal Vitamin C level and 32 in the high Vitamin C level. What is the NNT between normal and high supplemental Vitamin C groups?
17. During the COVID-19 pandemic several treatments were pushed by the public. For example, Dwayne “The Rock” Johnson pleaded for COVID-19 survivors to donate their plasma (Facebook video). On 23 August 2020, COVID-19 convalescent (“survivor’s”) plasma was approved for emergency use by FDA to treat patients with COVID-19 (FDA link). Researchers (Korley et al 2021) recruited 511 patients who presented to emergency departments with mild COVID-19 symptoms during first week after infection. Patients were randomly assigned to receive convalescent plasma treatment (n=257) or placebo treatment (n=254) to test whether survivor’s plasma prevented progression to severe COVID-19 illness. Disease progressed in 77 patients (30%) in the plasma treated group compared to 81 patients (31.9%) in the placebo group. Calculate RRR, the odds ratio, and NNT. Is “survivor’s” plasma a promising treatment?
Bonus questions
1. A doctor is about to inform a patient about results of her test for a disease. The disease has 1 in 1000 prevalence in the population. The test to detect the disease has a false positive rate of 5 percent. The patient’s test result is positive. What are the chances the patient has the disease? (be able to show your work!!)
- 5%
- 10%
- 25%
- 50%
- 95%
2. A surgeon In Michigan advocated removing the breasts of healthy women if they fall into a high-risk group. His argument goes something like this (this example is from Gerd Gugerenzer’s book, Calculated Risks):
- 57% of women in the general population are at high risk for developing breast cancer
- 92% of all breast cancers are found in this group
- 1 in 13 women in the general population (both low and high risk) develops breast cancer between ages 40 and 59
- Therefore, 1 in every 2 or 3 women in the high-risk group will develop breast cancer between ages 40 and 59.
Based on these arguments, he removed the “high-risk” breasts of 90 cancer-free women, replacing them with implants.
2A) Calculate ARR, RRR, and NNT
2B) Is the surgeon’s reasoning correct? Work through his numbers in points 1 – 4 and see if there are defects in his logic. Your answer will address, How many high-risk women are likely to develop breast cancer?
3. When a man turns 50, two things appear in the mailbox: An invitation to join AARP and a FOBT kit from his health care provider. FOBT is an inexpensive, painless screening tool for colorectal cancer (CRC). The traditional version (gFOBT) is based on a guaiac spot on a test strip, whereas the newer version (fecal immunochemical test or FIT) is based on two monoclonal antibodies. The sensitivity of gFOBT is 51%, the sensitivity of FIT is 75%; specificity of gFOBT is 78%, the specificity of FIT is 90%. Given that the prevalence of CRC in men between 50 and 59 is about 0.2%, please evaluate the value of FOBT testing for CRC in this age group
3A) In this age group, how many men are expected to develop CRC?
3B) How many positive tests are likely to be true positives?
3C) How many false negative would we expect?
3D) What is the NNT for FIT compared to gFOBT?
References
Akolekar, R., Beta, J., Picciarelli, G., Ogilvie, C., & D’Antonio, F. (2015). Procedure‐related risk of miscarriage following amniocentesis and chorionic villus sampling: a systematic review and meta‐analysis. Ultrasound in Obstetrics & Gynecology, 45(1), 16-26.
Centers for Disease Control and Prevention. (2021, August 3). FastStats – Births and Natality. Centers for Disease Control and Prevention. Retrieved October 12, 2021, from https://www.cdc.gov/nchs/fastats/births.htm
Gigerenzer, G. (2015). Calculated risks: How to know when numbers deceive you. Simon and Schuster.
Korley, F. K., Durkalski-Mauldin, V., Yeatts, S. D., Schulman, K., Davenport, R. D., Dumont, L. J., … & Callaway, C. W. (2021). Early convalescent plasma for high-risk outpatients with Covid-19. New England Journal of Medicine.
Manson, J. E., Chlebowski, D. R. T., Stefanick, M. L., Aragaki, M. A. K., Rossouw, J. E., Prentice, R. L., … & Wallace, R. B. (2013). The Women’s Health Initiative hormone therapy trials: update and overview of health outcomes during the intervention and post-stopping phases. JAMA: the journal of the American Medical Association, 310(13), 1353.
Martin, J. A., Hamilton, B. E., Osterman, M. J., & Driscoll, A. K. (2021). Births: Final Data for 2019. National Vital Statistics Reports: From the Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System, 70(2), 1-51.
Tverdal, A., Hjellvik, V., & Selmer, R. (2011). Coffee intake and oral–oesophageal cancer: follow-up of 389 624 Norwegian men and women 40–45 years. British journal of cancer, 105(1), 157-161.
/MD